Barking Up the Wrong Tree: MASH, Fatty Liver, and the Statin Blame Game
MASH, Fatty Liver, and the Statin Blame Game
Case Presentation
A 54-year-old man with obesity (BMI 32), hypertension, and "borderline high cholesterol" is started on atorvastatin after his primary care physician calculates a 10-year cardiovascular risk of 12%. Six weeks later, routine labs show his ALT is mildly elevated at 58 U/L (normal <40). His LDL-C has dropped beautifully from 142 to 78 mg/dL.
His doctor says: "Your liver enzymes are up. It might be the statin. Let's stop it and recheck in a month."
A month later, his ALT is… still 52 U/L. The statin wasn't the cause. But now his LDL-C has bounced back to 136 mg/dL, and nobody has restarted it.
Two years later, he presents with chest pain. A cardiac catheterization reveals severe three-vessel coronary artery disease. He undergoes bypass surgery.
Looking back at his records, his ALT had actually been mildly elevated for years — even before the statin was started. Nobody noticed. Nobody investigated.
He had fatty liver disease all along. And his statin — wrongly blamed and stopped — might have helped prevent his heart disease.
A 47-year-old woman with metabolic syndrome — waist circumference 38 inches, triglycerides 220 mg/dL, HDL-C 38 mg/dL, fasting glucose 112 mg/dL, blood pressure 138/88 mmHg — sees her gastroenterologist for "abnormal liver tests." Her AST is 45 U/L and ALT is 62 U/L.
An ultrasound shows "hepatic steatosis." The gastroenterologist tells her: "You have fatty liver. Try to lose some weight. We'll recheck in 6 months."
No one tells her that fatty liver is a cardiometabolic disease. No one calculates her cardiovascular risk. No one checks her ApoB. No one screens for sleep apnea. No one refers her to cardiology.
Three years later, she has a heart attack at age 50.
Her hepatologist had been watching her liver. No one was watching her heart. Her fatty liver was a warning sign of the cardiovascular disease that almost killed her.
A 61-year-old man with type 2 diabetes, hypertension, and obesity is told he has "NASH" after a liver biopsy shows steatohepatitis with stage 2 fibrosis. He's referred to a hepatologist who focuses on monitoring for progression to cirrhosis.
Meanwhile, his diabetes is poorly controlled (HbA1c 8.2%), his triglycerides are 280 mg/dL, his HDL-C is 34 mg/dL, and he's sedentary. He takes metformin but no other diabetes medications. He's on a low-dose statin but his ApoB has never been checked.
His hepatologist says: "We need to watch for cirrhosis. Get a FibroScan every year."
But no one is aggressively treating his diabetes. No one has considered a GLP-1 agonist that could help his weight, his glucose, AND his liver. No one has optimized his lipid therapy. No one has prescribed structured exercise. They're watching the liver while ignoring the cardiometabolic fire that's burning it.
Flying Under the Radar
Metabolic dysfunction-associated steatotic liver disease (MASLD) — what we used to call "non-alcoholic fatty liver disease" (NAFLD) — has become the most common chronic liver disease worldwide. According to a comprehensive review in the New England Journal of Medicine (Targher G et al., N Engl J Med 2025;393:683–698), MASLD affects approximately 30-40% of the general adult population globally, including 60-70% of individuals with type 2 diabetes and 70-80% of those with obesity.
And yet it remains dramatically underdiagnosed, undertreated, and misunderstood.
Why does fatty liver fly under the radar?
The Statin Blame Game
When a patient on a statin has mildly elevated liver enzymes, the reflexive response is often: "Stop the statin."
This is almost always barking up the wrong tree.
The National Lipid Association's Statin Liver Safety Task Force (Jacobson TA, J Clin Lipidol 2014) addressed this directly, concluding that:
- Statins rarely cause clinically significant liver injury. True statin hepatotoxicity is exceedingly rare — estimated at approximately 1 per 100,000 patient-years
- Routine periodic monitoring of liver enzymes does not appear to be effective in detecting or preventing serious liver injury
- Mild, asymptomatic elevations of hepatic transaminases are common with statin therapy but are usually benign and do not predict serious liver injury
- Statins can be used safely in patients with chronic liver disease, including NAFLD — and these patients may actually benefit the most
Based on this evidence, the FDA changed statin labeling in 2012, removing the requirement for routine liver enzyme monitoring. The FDA concluded that "serious liver injury with statins is rare and unpredictable in individual patients, and that routine periodic monitoring of liver enzymes does not appear to be effective in detecting or preventing serious liver injury."
The bottom line: If a patient on a statin has mildly elevated liver enzymes (<3x upper limit of normal), fatty liver is far more likely to be the cause than statin toxicity. And stopping the statin removes cardiovascular protection from a patient who likely needs it most.
A Disease Without Symptoms
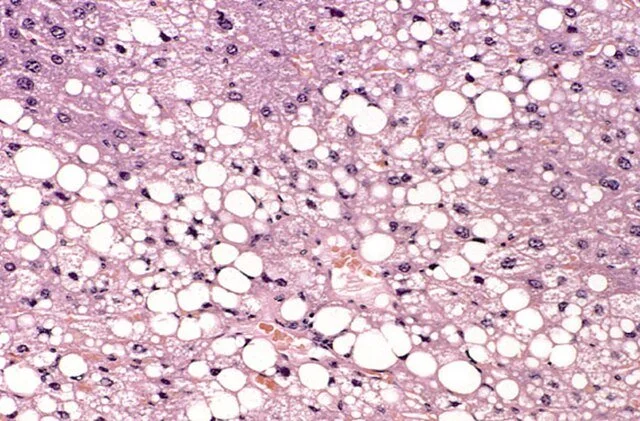
Fatty liver is silent. It doesn't hurt. It doesn't cause jaundice until it's far advanced. Patients feel fine while their liver accumulates fat, develops inflammation, and slowly scars.
By the time symptoms appear — fatigue, abdominal discomfort, signs of portal hypertension — the disease has often progressed to cirrhosis.
Specialty Fragmentation
Who owns fatty liver?
- Gastroenterologists and hepatologists see it as a liver disease — they watch for cirrhosis
- Endocrinologists see it as a complication of diabetes
- Cardiologists often don't think about the liver at all
- Primary care may dismiss it as benign or blame medications
The result: The cardiometabolic disease driving fatty liver goes undertreated, while everyone watches and waits for the liver to get worse.
The Wrong Name for Decades
For years, we called it "Non-Alcoholic Fatty Liver Disease" (NAFLD) — defining it by what it isn't (not caused by alcohol) rather than what it is (caused by metabolic dysfunction).
The 2023 multi-society Delphi consensus statement (Rinella ME et al., Hepatology 2023) introduced new terminology — MASLD (Metabolic dysfunction-Associated Steatotic Liver Disease) and MASH (Metabolic dysfunction-Associated Steatohepatitis) — correctly emphasizing that this is a metabolic disease, not merely a liver abnormality.
This matters because the treatment isn't "liver therapy." The treatment is addressing the metabolic dysfunction.
The #1 Killer Is Not Liver Failure
Here's the statistic that changes everything:
The NEJM review (Targher G et al., 2025) confirms that the presence of MASLD is associated with increased morbidity and mortality due to liver-related complications, hepatocellular carcinoma, cardiovascular disease, and certain extrahepatic cancers. A landmark meta-analysis by Mantovani et al. (Lancet Gastroenterol Hepatol 2021) established that cardiovascular disease — not liver failure — is the leading cause of death in patients with fatty liver disease. Two major 2026 practice guidelines — from the Japan Society of Hepatology and the Italian Association for the Study of the Liver — reaffirm this point and explicitly call for cardiologists to be integral partners in multidisciplinary MASLD care. In May 2026, the AACE Type 2 Diabetes Algorithm took the most significant structural step yet: elevating MASLD to stand alongside heart failure, CKD, and ASCVD as a core complication requiring active screening (FIB-4) and driving therapeutic selection — the first major U.S. diabetes guideline to formally place liver disease on equal footing with cardiovascular and renal disease. Preferred agents when MASLD is present: GLP-1 receptor agonists and pioglitazone; resmetirom (Rezdiffra) is referenced for MASH with significant fibrosis.
Fatty liver isn't just a marker of metabolic dysfunction. It may actively contribute to atherosclerosis through:
- Increased production of atherogenic lipoproteins (VLDL, small dense LDL)
- Systemic inflammation
- Insulin resistance
- Prothrombotic state
Watching fatty liver without aggressively treating cardiovascular risk is watching the wrong endpoint.
Biomarkers That Link Liver and Heart Risk
If you have MASLD, your liver health and heart health are interconnected. Simple blood tests can help identify how much cardiovascular risk your liver disease is adding.
FIB-4: A Liver Test That Predicts Heart Disease
The FIB-4 index — calculated from your age, platelet count, and liver enzymes (AST and ALT) — was originally developed to detect liver fibrosis. But research now shows it also predicts major adverse cardiovascular events independently (Vieira Barbosa et al., Am J Gastroenterol 2022), even after accounting for traditional risk factors like cholesterol and blood pressure.
In a large Korean study of over 60,000 participants (Lee & Lee, Sci Rep 2025), elevated FIB-4 was significantly associated with coronary artery calcification progression — a marker of subclinical atherosclerosis.
This is a critical gap in current practice: standard cardiovascular risk calculators don’t account for liver fibrosis — even though fibrosis stage predicts cardiovascular events independently of traditional risk factors. New research has begun to address this directly: the LIVER-ASCVD+ model, published in the Journal of Hepatology (2026), integrates liver biomarkers (including FIB-4 and liver stiffness) with traditional cardiovascular risk factors to improve 10-year ASCVD prediction specifically in MASLD patients — reclassifying a meaningful proportion into higher-risk categories who would otherwise be undertreated by standard calculators alone.
Liver Stiffness and Atherosclerosis
Liver stiffness measurements — via FibroScan (transient elastography) or MR elastography — don't just tell you about fibrosis. They also correlate with subclinical atherosclerosis. In diabetic patients, liver stiffness was associated with increased cardiovascular risk (Mangla N et al., Clin Gastroenterol Hepatol 2020).
Inflammatory Markers
Data from the ARIC (Atherosclerosis Risk in Communities) study (Wang JJ et al., J Inflamm Res 2024) show that monocyte counts and hsCRP predict 10-year cardiovascular events specifically in MASLD patients. This reinforces that fatty liver is an inflammatory state — and inflammation drives both liver progression and atherosclerosis.
The Fibrotic NASH Index (FNI)
The FNI — derived from AST, HbA1c, and HDL-C — has been endorsed by the European Atherosclerosis Society for identifying high-risk MASLD patients who warrant aggressive cardiovascular prevention.
The bottom line: Knowing your fibrosis stage may be as important for your heart as it is for your liver. If you have MASLD, ask your clinician whether FIB-4 or liver stiffness testing makes sense for you.
The Usual Suspects
Fatty liver doesn't appear alone. It travels with a familiar constellation of cardiometabolic conditions — the "usual suspects" that cluster together and amplify each other's damage.
Insulin Resistance & Dysglycemia
Insulin resistance is the central driver of fatty liver. When cells become resistant to insulin's effects:
- The liver ramps up de novo lipogenesis — synthesizing fat from carbohydrates
- Adipose tissue releases more free fatty acids, which flood the liver
- The liver becomes overwhelmed and stores excess fat as triglyceride
The progression: insulin resistance → prediabetes → type 2 diabetes → worsening fatty liver → increased cardiovascular risk.
The Atherogenic Triad
Fatty liver is intimately connected to the Atherogenic Triad — consisting of:
- Elevated triglycerides — the liver overproduces VLDL particles
- Low HDL-C — triglyceride-rich lipoproteins exchange with HDL, reducing HDL cholesterol
- Small, dense LDL particles — more numerous than LDL-C suggests, creating discordance between LDL-C and true atherogenic particle burden (ApoB)
This is why ApoB is so important in fatty liver patients. LDL-C may look "normal" while particle number (ApoB) is dangerously elevated.
Visceral Adiposity — "Sick Fat"
Not all fat is created equal. Subcutaneous fat (under the skin) is relatively benign. Visceral fat — the fat that accumulates in and around organs, including the liver — is metabolically toxic.
Visceral adipose tissue is "sick fat" (adiposopathy) — or as we call it at CardioAdvocate, "pissed off fat." A landmark 2025 JACC State-of-the-Art Review by Dr. Milton Packer now formalizes this concept as the "Adipokine Hypothesis," showing that dysfunctional visceral fat secretes an altered suite of signaling molecules (adipokines) that drive inflammation, fibrosis, and metabolic disease across multiple organs — including the liver, heart, and kidneys. MASLD/MASH, HFpEF, type 2 diabetes, and chronic kidney disease are not independent conditions that happen to coexist; they are downstream manifestations of the same adiposopathic source.
- Secretes pro-inflammatory cytokines
- Promotes insulin resistance
- Contributes to systemic inflammation and oxidative stress
- Directly deposits fat in the liver
Waist circumference — not BMI alone — is a key marker of visceral adiposity and fatty liver risk. Packer's work confirms that central adiposity — measured by waist-to-height ratio (≥0.5) — is the most reliable indicator of the adipokine dysregulation that drives both hepatic steatosis and cardiac disease. This is why GLP-1 receptor agonists like semaglutide and SGLT2 inhibitors show benefits across MASLD, HFpEF, and diabetes simultaneously — they are targeting the same upstream driver: adiposopathy.
Metabolic Syndrome
Fatty liver is essentially the hepatic manifestation of metabolic syndrome. The criteria are:
- Waist circumference: >40" (men), >35" (women)
- Triglycerides ≥150 mg/dL
- HDL-C <40 mg/dL (men), <50 mg/dL (women)
- Blood pressure ≥130/85 mmHg
- Fasting glucose ≥100 mg/dL
If you have three or more of these, you have metabolic syndrome — and you very likely have fatty liver.
Sedentary Lifestyle
Physical inactivity promotes fatty liver through multiple mechanisms:
- Reduced insulin sensitivity
- Decreased muscle uptake of glucose and fatty acids
- Increased hepatic fat accumulation
- Loss of metabolically active muscle mass
The flip side: Exercise improves fatty liver even without weight loss. Both cardio and resistance training have independent benefits.
Sleep Apnea & Poor Sleep
Obstructive sleep apnea (OSA) is strongly associated with fatty liver (Mesarwi OA et al., Am J Respir Crit Care Med 2019):
- Intermittent hypoxia promotes hepatic inflammation and fibrosis
- Sleep deprivation worsens insulin resistance
- OSA and fatty liver share common risk factors (obesity, metabolic syndrome)
Patients with fatty liver should be screened for OSA.
Alcohol: The Original Suspect (But Not the Only One)
The new MASLD terminology doesn't mean alcohol is irrelevant. Alcohol and metabolic dysfunction can coexist — and their effects on the liver are additive.
Even "moderate" alcohol consumption worsens fatty liver in patients with metabolic dysfunction. For many patients with MASLD, alcohol reduction or elimination should be part of treatment.
CardioAdvocate Checklist
If you have fatty liver — or elevated liver enzymes — ask these questions:
Challenge the Statin Blame
Get Properly Evaluated
Screen for the "Usual Suspects"
Address Cardiovascular Risk
Questions to Ask Your Clinician
- "Could my elevated liver enzymes be from fatty liver rather than my statin?"
- "I have fatty liver. Has my FIB-4 score been calculated?"
- "Does my liver fibrosis stage affect my cardiovascular risk?"
- "Should I have liver stiffness measured with elastography?"
- "Should my ApoB be checked?"
- "Are there medications that would help both my liver AND my heart?"
- "Who is coordinating my care for fatty liver and cardiovascular risk?"
Deep Dive
Lifestyle: The Foundation of Treatment
Lifestyle modification remains the cornerstone of therapy — and the evidence is compelling.
Weight Loss
- Weight loss of 7-10% significantly reduces liver fat and inflammation (Promrat K et al., Hepatology 2010)
- Weight loss of ≥10% can improve or even resolve fibrosis in some patients
- Weight fluctuation (yo-yo dieting) may be harmful; sustained weight management is key
Exercise
Exercise improves fatty liver even without significant weight loss (Hallsworth K et al., Gut 2011):
- Aerobic exercise (walking, cycling, swimming) — 150+ minutes per week improves hepatic steatosis
- Resistance training — builds metabolically active muscle, improves insulin sensitivity, and independently benefits the liver
- Combined cardio + resistance training provides the greatest benefit
The message: Move more. Lift things. Do both.
Diet
No single "liver diet" has been proven superior, but principles that help:
- Mediterranean diet — associated with reduced hepatic steatosis and improved insulin sensitivity (Ryan MC et al., J Hepatol 2013)
- Reduce refined carbohydrates and added sugars — these drive hepatic de novo lipogenesis
- Limit fructose — particularly from sugary beverages, which directly promote liver fat
- Adequate protein — supports muscle mass and satiety
- Moderate caloric restriction — to achieve weight loss
Sleep
Poor sleep worsens insulin resistance and metabolic dysfunction. Addressing sleep quality and treating sleep apnea are important components of fatty liver management.
Alcohol
For patients with metabolic fatty liver, alcohol adds injury on top of injury. Reduction or elimination is recommended, particularly for those with steatohepatitis or fibrosis.
Pharmacotherapy: Treating the Underlying Disease
The NEJM review (Targher G et al., 2025) highlights that pharmacotherapies now target both liver and cardiovascular-renal-metabolic issues simultaneously:
Statins
- Safe in fatty liver — the NLA Statin Liver Safety Task Force (2014) explicitly states statins can be used safely in patients with chronic liver disease including NAFLD
- Reduce cardiovascular risk — the #1 cause of death in fatty liver patients
- Some data suggest statins may modestly improve liver histology
- Guidelines recommend statins in fatty liver patients who meet cardiovascular indications
GLP-1 Receptor Agonists (semaglutide, tirzepatide, liraglutide)
These are transforming fatty liver treatment. Subcutaneous semaglutide resolved NASH in 59% of patients vs 17% placebo in a Phase 2 trial (Newsome PN et al., N Engl J Med 2021), and is now conditionally FDA-approved for adults with MASH who have moderate to advanced fibrosis:
- Promote significant weight loss
- Improve glycemic control
- Directly improve hepatic steatosis and inflammation
- Tirzepatide (dual GIP/GLP-1 agonist) shows even greater weight loss and metabolic benefit
- Provide dual benefit for liver AND cardiovascular outcomes
Pioglitazone
- Insulin sensitizer (thiazolidinedione)
- Improves steatohepatitis in clinical trials (Sanyal AJ et al., PIVENS Trial, N Engl J Med 2010)
- Guideline-recommended option for NASH, particularly in diabetic patients
- Concerns: weight gain, fluid retention, bone loss — discuss risks/benefits
SGLT2 Inhibitors (empagliflozin, dapagliflozin, etc.)
- Cardiovascular and renal benefits well-established
- Emerging evidence of liver benefit in MASLD
- Reasonable option for patients with diabetes and fatty liver
- Provide dual benefit for liver AND cardiovascular-renal outcomes
Vitamin E
- Antioxidant that improves NASH histology in some trials
- Recommended as an option in non-diabetic NASH patients
- Long-term safety concerns (prostate cancer, bleeding) — use with caution
Resmetirom (Rezdiffra)
The MAESTRO-NASH trial (Harrison SA et al., N Engl J Med 2024) established resmetirom (a liver-directed, thyroid hormone receptor β-selective agonist) as the first FDA-approved medication specifically for MASH (March 2024):
- First FDA-approved medication specifically for MASH (March 2024)
- Achieved NASH resolution in 26-30% of patients vs. 10% on placebo
- Achieved fibrosis improvement in 24-26% vs. 14% on placebo
- Represents a new era of targeted liver therapy
The Cardiovascular Imperative
We cannot overstate this: Fatty liver patients die from heart disease more than liver disease.
This means cardiovascular risk assessment and treatment are not optional extras — they are central to fatty liver management:
- Calculate cardiovascular risk — and recognize that fatty liver adds risk beyond standard calculators
- Calculate FIB-4 — fibrosis stage predicts cardiovascular events independently
- Check ApoB — LDL-C underestimates risk when triglycerides are elevated (common in fatty liver)
- Treat aggressively — statins are first-line; add ezetimibe if needed; consider PCSK9 inhibitors for very high risk
- Control blood pressure — hypertension is common in metabolic syndrome
- Screen for and treat diabetes — GLP-1 agonists and SGLT2 inhibitors offer dual liver-heart benefit
Monitoring and Follow-Up
Patients with fatty liver need long-term monitoring:
- Liver fibrosis assessment — FibroScan or other non-invasive markers every 1-2 years; use the FIB-4 calculator as a screening tool
- Metabolic parameters — weight, waist circumference, glucose, HbA1c, lipid panel, ApoB
- Cardiovascular risk assessment — ongoing attention to CV prevention; remember FIB-4 predicts CV risk too
- Progress with lifestyle changes — support for diet, exercise, alcohol reduction
- Response to therapy — are medications helping?
When liver enzymes are mildly elevated, don't bark up the statin tree. The real culprit is almost always metabolic dysfunction — and fatty liver is its hepatic manifestation.
Fatty liver is not a benign condition to "watch." It's a warning sign of systemic cardiometabolic disease that demands action.
The treatment is not liver-specific. It's addressing the usual suspects: insulin resistance, atherogenic dyslipidemia, visceral adiposity, sedentary lifestyle, poor sleep, and excess alcohol.
Statins are not the enemy — they're part of the solution. The National Lipid Association's Statin Liver Safety Task Force made this clear over a decade ago: statins are safe in fatty liver, and these patients benefit the most from cardiovascular protection.
New medications like GLP-1 agonists, SGLT2 inhibitors, and resmetirom are changing the treatment landscape — many offering dual benefit for both liver and cardiovascular outcomes. But lifestyle remains the foundation: sustained weight loss, exercise (cardio AND resistance), healthy diet, better sleep, and alcohol moderation.
Your liver fibrosis stage may predict your heart risk as much as your cholesterol does. If you have fatty liver, ask who is coordinating your care. Ask about your FIB-4 score. Ask about your cardiovascular risk. Ask about your ApoB. Ask whether you're being treated aggressively enough.
Your liver is telling you something important about your whole body. Make sure someone is listening.
CardioAdvocate helps people understand what matters — and how to speak up about it.
Content on CardioAdvocate.com is for educational purposes only and does not constitute medical advice. No physician–patient relationship is created. Always consult a qualified healthcare professional for medical concerns.